This episode is not available for CEUs through the Sound Bites Podcast. However, there will be a CEU opportunity available through Today’s Dietitian in the near future. Please visit the Today’s Dietitian site or check back here for further details to be shared when they are available.
Irritable Bowel Syndrome: The Gut, Brain and Food Connection
If you have been living with IBS (or other GI conditions) and don’t feel like you are living well – consider a treatment plan that addresses your nutrition as well as your mental health. Our book is a fantastic resource to guide you to specific nutrition and behavioral health strategies that are backed by science.” – Dr. Megan Riehl
There are many factors that impact gut health: diet, mental health, genes, exercise, and more. Many of these factors can be changed to improve overall health via the gut. Mental health and the role of stress is important to consider in the management of one’s physical health and may become an important target of treatment.
Irritable Bowel Syndrome is a chronic GI condition that presents with abdominal pain and alterations in bowel habits and is diagnosed based on symptoms after ruling out other conditions such as Inflammatory Bowel Disease.
GI conditions, such as IBS, often require medical management in addition to food, mood and lifestyle changes.
The newly released book, Mind Your Gut: The Science-based, Whole-body Guide to Living Well with IBS is an evidence-based toolkit that will help readers understand the ins and outs of IBS, the available treatment options and key strategies that can be implemented right away.
Tune into this episode to learn about:
Gut health in general
How stress impacts health
How a GI psychologist is different from a general mental health provider
What IBS is, how it develops and how it is diagnosed
The newly released book: Mind Your Gut
The gut, brain and food connection
Nutritional and behavioral strategies to manage IBS
Common IBS myths
Lifestyle factors to improve gut health and overall health
I give you this background to certify that Kate and Megan are the real deal. They’re not just experts, they helped create and shape their respective fields. They bring all their experience to bear in Mind Your Gut. The book rightfully presents food and stress as codependent influences in the pathogenesis and treatment of IBS. I’m confident that the strategies in this book will help you be more confident in managing your IBS, enabling you to take back control of your life.” – Dr. William Chey, Chief of Gastroenterology, Michigan Medicine
Megan Riehl, PsyD, MA, AGAF
Dr. Megan Riehl is an Associate Professor of Medicine and Director of GI Behavioral Health at the University of Michigan where she has a full-time clinical practice, leads GI behavioral health trainings, and provides mentorship and consultation. Her clinical expertise spans the field of gastroenterology from those living with IBS to those with chronic gastrointestinal diseases. Dr. Riehl actively engages on multiple national committees focused on improving the psychological well-being of individuals with GI conditions. Her research and passion for education has resulted in numerous peer-reviewed publications, leadership roles, and international speaking engagements.
Kate Scarlata, MPH, RDN
Kate Scarlata is a US-based dietitian with 30+ years of clinical experience. Kate’s expertise is in gastrointestinal disorders and food intolerance. She was awarded the Outstanding Massachusetts Dietitian Award and recognized as Boston’s Best Dietitian by Boston Magazine. Kate is the co-author of numerous books and articles on digestive health topics including Mind Your Gut with Dr. Megan Riehl (pub date March 5, 2024), the New York Times Best Seller, The 21 Day Tummy Diet, and The Low FODMAP Diet Step by Step. Kate completed her postgraduate training at Brigham and Women’s Hospital, a Harvard Medical School teaching affiliate, and her master’s degree in public health at University of Massachusetts. In addition to her clinical work, Kate’s patient advocacy work includes her #IBelieveinyourStory campaign raising awareness of IBS, sharing patient’s lived experiences, and securing funding for IBS research as well as her #EndHungerPain initiative where Kate partnered with food manufacturers to provide special diet foods to food pantries. The #EndHungerPain initiative increased attention to the many challenges of living at the intersection of gluten free and low FODMAP diet needs while food insecure.
Resources
Some links may be affiliate links. As an Amazon Associate, I earn from qualifying purchases.
Speakers: Melissa Joy Dobbins, Kate Scarlata, & Megan Riehl
[Music Playing]
Voiceover (00:00):
Welcome to Sound Bites, hosted by Registered Dietitian Nutritionist, Melissa Joy Dobbins. Let’s delve into the science, the psychology, and the strategies behind good food and nutrition.
Melissa Joy (00:22):
Hello, and welcome to the Sound Bites Podcast. Today’s episode is about IBS, irritable bowel syndrome. And we’ll also touch on general gut health as we begin our conversation, and then discuss nutrition and behavioral health strategies for managing IBS.
My guests today are Dr. Megan Riehl, and dietitian, Kate Scarlata. They are co-authors of the newly released book, Mind Your Gut: The Science-based, Whole-body Guide to Living Well with IBS.
Dr. Megan Riehl has a doctorate in psychology, a master’s in clinical counseling, and is a fellow of the American Gastroenterological Association. She’s an associate professor of medicine and director of GI Behavioral Health at the University of Michigan, and has numerous peer reviewed publications, leadership roles, and international speaking engagements.
Kate Scarlata is a Boston-based registered dietitian with more than 30 years of clinical experience in digestive health and GI disorders. She completed her postgraduate training at Brigham and Women’s Hospital and her master’s degree in public health at the University of Massachusetts, and she’s been on the podcast twice before talking about gut health.
I want everybody listening to know that this episode is not sponsored.
Ladies, welcome to the show.
Kate Scarlata (01:45):
Thanks for having us.
Megan Riehl (01:46):
Thank you so much. What a nice introduction.
Melissa Joy (01:50):
So thrilled to have you on and dive into this very important topic, gut health in general. I mean, we’re not going to gloss over that. We’re going to talk about that quite a bit because that impacts everybody. But also, IBS more specifically, and of course, your new book.
So, I’d love for both of you to share more about your background, your education, and the work you do, how you got interested in digestive health, and also, of course, any disclosures to note.
Kate, let’s start with you.
Kate Scarlata (02:16):
Awesome. So, I’ve been a dietitian for a million years, but about 30 years ago what sort of segued me over to the digestive health and GI space was a personal health scare. I was pregnant with my middle son and developed this colicky stomach pain that my OB-GYN said, “Come in, we really should take a look.”
And long story short, I had scar tissue that was strangulating my small intestine and really cutting off the blood supply. So, my intestine was dying inside of me while I was trying to grow a baby, and it was a pretty serious event.
But what really pushed me into the digestive health space was I was discharged with eight feet of my small intestine removed and so many GI symptoms, and they basically said, “Just eat a steak. Good luck.”
And I’m growing a baby and I have this huge scar on my belly, and I’m trying to feel well and nourish my body and the baby I’m growing. And I realized, wow, I really need to learn more about this.
And so, that really jet-setted me into the digestive health space. And I was really a fanatic about reading everything in the scientific literature and really just trying to understand the gut microbiome and understand food related to intestinal resections.
And that kind of segued me into IBS education, and in all of my learning is when I stumbled across the low-FODMAP diet kind of emerging in the research, and I thought, “Wow, these foods are really the list of foods that are problematic for me. This is interesting.”
And that segued me down to Australia. I visited with Monash University researchers, I wanted to know everything that they were doing. I knew this was an important diet therapy, and it’s proven to be the most evidence-based for IBS. So, I guess I was right about that. But it really put me in the forefront.
So, I was a general dietitian initially, and then as I started a blog and talking about digestive health and the FODMAP diet, my full-time practice became all GI patient.
And so, that landed me here, and I’ve never looked back. It’s been such a rewarding space to work in. I’ve been able to really take this area and do what I want with it and things that are passionate to me, like food insecurity, and how do people with food insecurity get special diet foods like low-FODMAP or gluten-free foods — they’re so expensive. And started an initiative called the End Hunger Pain Initiative, where we got lots of different foods through Schär and Fody, who I have sponsored partnerships with.
They loaded this AirStream, and I brought it down the East Coast, hit up a lot of different food pantries where we were really raising awareness that people with special diet needs need help. If they’re financially strapped, this is adding an extra layer. So, that’s one area that I’ve been able to sort of bring my passion to the world, so to speak.
And then I also started another campaign called the I Believe in Your Story Campaign, because when I was hospitalized, quite frankly, the doctors didn’t believe me. They thought I was pain-seeking. And this happens to a lot of women and IBS affects more women than men, and a lot of them are gaslit or not really heard, and I wanted them to have a safe space to be heard.
And so, I started the I Believe in Your Story Campaign to really raise awareness for IBS, raise research funding, which is really minimal. It’s about 11 cents per IBS patient for NIH funding, and provide a safe space for them to share their story to feel believed.
There’s a lot I could talk about. 30 years is a long time, but that’s a quick and probably somewhat, long elevator speech about what I’ve been doing.
Melissa Joy (06:31):
Thank you. Yes, and I guess it was episode 201 where we did talk about that intersection of food insecurity and food intolerance, and some of what you touched on. So, if anybody’s interested, I’ll have a link in my show notes, and they can take a deeper dive into that or just look it up.
And I’m sure we touched on FODMAP with the other episode that you were on, and you’ve authored several books. Do you want to name those real quickly?
Kate Scarlata (06:54):
Oh, my goodness. So, yeah, I’ve had five books. So, I started with The Complete Idiot’s Guide to Eating Well with IBS, and then that segued me into working with Reader’s Digest. I co-authored the 21-Day Tummy Diet, and that became a New York Times bestseller, which was very cool. And then I followed up with a recipe book for the 21-Day Tummy Diet, also with Reader’s Digest.
And then more recently, I did The Low-FODMAP Diet Step by Step, which is all about FODMAPs with Dede Wilson, who is a Bon Appetit editor and recipe developer. So, that was really cool.
And then the best of all, I collaborated with the lovely Dr. Riehl to do Mind Your Gut, which is really been a dream of mine for a very long time. I wanted a full toolkit for IBS patients, so they would have lots of different treatments available to them because IBS is very complex. It’s not one size fits all in patients, or people living with this condition really need a lot of tools. So, that’s hot off the press.
Melissa Joy (08:00):
That’s right.
Kate Scarlata (08:01):
So, exciting.
Melissa Joy (08:02):
And Dr. Megan Riehl, let’s hear a little bit about your backstory.
Megan Riehl (08:06):
Well, Kate and I, we work pretty closely together, but every time she shares her story, I’m that much more inspired. I’m that much more appreciative to the work, dedication, effort, thought, time — all these initiatives take so much emotional and physical strength and resilience to take really an idea and put it literally driving down the coast. So, I’ve got an absolute dream in a partner with Kate.
So, to go a little bit back in my journey to being a GI psychologist and sitting here as a co-author with Kate … you asked for it, so I’m going to give you the real history here.
Melissa Joy (08:50):
Great.
Megan Riehl (08:51):
Not long ago, my mom sent me a text of a picture of what I wanted to be when I grew up in second grade, and I wrote that I wanted to be a psychologist. So, from a very early age, I knew
So, I knew it from a very early age for a couple different reasons. One being that my brother and I, we took very different paths in life with the same amazing parents. So, he was somebody that would break apart an engine at 10-years-old and put it back together. And that stressed me out and made me anxious.
So, I was always interested in how his mind worked. And so, then I went to Michigan State University for undergrad, kind of forgetting I wanted to be a psychologist and thinking I wanted to be an attorney.
And very quickly, determined I don’t want to be an attorney. And so, my sophomore year, I said, “Wait a minute, I wanted to be a psychologist. How do I do that?”
And so, I scheduled a couple psychology courses, reached out to a couple psychologists doing clinical research at Michigan State. I asked to meet with them to learn a little bit more about a couple things that they were doing that I thought were interesting and joined a lab.
I learned I didn’t want to do clinical research at an academic institution, but I was interested in psychology, I wanted to see patients. I wanted to do therapy, whatever my concept of that was as a sophomore.
And that took me to graduate school eventually. And I was in a graduate program that focused heavily on clinical training. And back at that time, there was a lot of kind of I don’t know, stigma about getting a Psy.D — that was different than going a PhD route.
A PhD route was very much, there would be only a couple slots at institutions, and you would do a lot of research. And I just knew in my gut that that wasn’t what I wanted to do. So, I was willing to go the Psy.D route that was very heavily focused on really learning how to be a clinician with patients.
And I think that hopefully, listeners will find this interesting, especially those in mental health, or those that are interested in potentially becoming a GI psychologist like myself. Because during my training, I was a generalist. I saw kids, I worked in corrections, I worked in prison settings in downtown Chicago. I worked in halfway houses with women transitioning from prison back into society.
I really saw almost any and every clinical diagnosis that you could think of, especially with a variety of people from diverse backgrounds. And I think that that’s so important when you’re going to subspecialize and, in my case, subspecialize and subspecialize and subspecialize.
So, it wasn’t until my internship that I began to kind of go into that intersection of health, physical health, and psychology.
And then as I was applying for fellowship opportunities, I kind of really wanted to stay in the Chicago land area, and this fellowship at Northwestern came up. And it was interesting. It was really the only fellowship that had specific GI behavioral health training within a gastroenterology division. And I thought, “Well, that’s interesting.”
And to be very honest, I can say this now without feeling ashamed, but I didn’t even know the difference really, between IBS and inflammatory bowel disease, IBD. But I figured I can learn, and as long as I am not harming anybody, I can figure this out.
So, I did a one-year fellowship, and that quickly turned into two years, and it quickly turned into a love for this field because I got to apply these psychological interventions that I knew well to the management of GI conditions, and people got better.
And a lot of times people would say, “Where the heck were you three, four, five experts before?” I really needed this collaborative approach with a gastroenterologist and a psychologist. And at Northwestern, they still have a fabulous dietitian (shout out to Beth Doerfler).
And I think that I learned too, wow, I could have an opportunity to shape this field a little bit with the genius of my mentors, but it was such a small field that I figured, wow, I’ve got an opportunity to sit at the table for this, I’m going to sit.
And so, then I got hired at the University of Michigan to develop their GI behavioral health program. I created a training program for other fellows so that we could help to increase access to GI behavioral health. And along the way, had a family and three kids and a book baby later.
Melissa Joy (14:53):
Excellent. Well, that leads me to my next logical question, and that is: how did the two of you meet and then subsequently decide to co-author this book?
Kate Scarlata (15:05):
So, I’ll start. Dr. Chey, William Chey, at U Michigan is incredible. And he started a nutrition course for dietitians interested in the GI space. And it’s called Food: The Main Course. And it is gone on now for several years, and I’ve been an invited guest, very fortunately. I feel like I’m like a sorority sister at U Michigan in some ways.
It’s been a lovely educational place for dietitians. And Megan, of course, being there was a speaker. And so, we had opportunities to kind of align and chat and sidebar, and that was sort of the beginning of our friendship. Could you have anything to add to that, Megan?
Megan Riehl (15:48):
No, no. She’s like an honorary faculty member at the University of Michigan. We’ve, I think, supported the I Believe in Your Story Campaign through our collaborative research. Kate has continued to contribute in different ways at U of M.
So, I had the privilege of kind of sitting in the audience listening to Kate as a sidebar before I’d give a talk, and really just her energy and having the opportunity to kind of watch this pioneer.
And then, I think I stalked her a little bit to say, “Hey, I have an idea.” And she gave it some thought and pause and made me wait on bated breath for a little while. And ultimately, we came together with a proposal for our book.
Melissa Joy (16:40):
Excellent. Well, you mentioned Dr. Chey, and I would love — we’re not going to talk about the book just yet, but I would love to read just the very last few sentences. He wrote the foreword for your book, and I really liked what he said. So, I wanted to just read this for our listeners.
He talks about the book and both of you and the very last few sentences say:
“I give you this background to certify that Kate and Megan are the real deal. They’re not just experts, they helped create and shape their respective fields. They bring all their experience to bear in Mind Your Gut.
The book rightfully presents food and stress as codependent influences in the pathogenesis and treatment of IBS. I’m confident that the strategies in this book will help you be more confident in managing your IBS, enabling you to take back control of your life.”
So, it’s by Dr. William Chey, the foreword of the book, and he’s the chief of gastroenterology at Michigan Medicine.
So, before we get more into the book and more possibly about the collaborative efforts that both of you, let’s talk about just what gut health is in general, what do our listeners need to know? And I know we’re going to talk about gut health throughout the rest of the conversation and more specifically, IBS. But what do we need to know to set the stage?
Kate Scarlata (18:03):
I’ll start and say that gut health is a very kind of general term, it’s definitely hot on TikTok these days. But when you really drill it down to the basics, it’s talking about the wellbeing of the digestive system and the trillions of microbes that reside in the gut.
And we know that when the gut bacteria and microbes are altered, we have a higher chance of having chronic disease. And when they’re beautifully balanced and playing well together, we have less risk of chronic disease.
We also know these microbes help us keep our immune system in check. They provide and produce vitamins for our body and help us digest fiber that escapes digestion. So, there’s so much that’s going on in our gut that play a big role in our overall health and wellbeing.
Melissa Joy (18:55):
Yeah, I remember learning even way back when I was in school, that our health and wellness depends on our gut health. If we don’t have good digestive health, we’re not going to be healthy overall. But that field has really evolved over my 30-year career as a dietitian as well.
And I know there’s a lot of different factors that impact gut health. Megan, maybe you want to speak to some of those.
Megan Riehl (19:18):
Yeah. So, gut health, it matters to all of us because so many different factors can impact it. We all have a brain, we all have a gut. And the brain gut connection is a very real bidirectional pathway that can be impacted by our nutrition, our lifestyle, meaning our sleep, our stress, our mental health, exercise.
So, recognizing that when we take a multidisciplinary approach for patients that may be struggling with their gut health, it’s because we each bring different strategies and tools to help you improve your overall health, which is ultimately going to affect gut health.
Melissa Joy (20:05):
Right. And seeing how you are the GI psychologist, which I know you talked a little bit about, but maybe you could also speak to how that’s different from just a general mental health provider. And maybe you covered that well enough already, but let’s talk about that stress and mental health impact. How does stress impact our physical health?
Megan Riehl (20:25):
Well, I think that’s a really good point that you make first, is the difference between somebody like myself, a GI psychologist, and somebody that’s a general mental health provider.
So, my role is to really hone in on strategies that are going to impact your gut health. So, I’m really helping patients with that kind of using brain gut behavioral therapies and helping with the management of their GI condition.
Now, patients that have, or people that have GI conditions like IBS and IBD have higher prevalences of anxiety and depression. That is true.
But if that anxiety and depression is more severe, then we really want them to work with a general mental health provider to first, stabilize those mood symptoms, the anxiety that may be related to their gut, but may also be related to several psychosocial stressors out there. At this point in the world, I think pretty much anyone can benefit from working with a therapist.
Melissa Joy (21:28):
Agree.
Megan Riehl (21:29):
And so, we really want somebody connected with a general mental health provider who’s going to cover the variety of things that are going on in somebody’s life.
So, one way I kind of help patients understand that is, let’s envision that you are driving a car, and the thing that’s in the front seat is your IBS or your IBD. If that’s the case, then working with somebody like me, if that passenger is your GI health or the things that are impacting your GI health, then come see me.
But if that is something that’s in the car, but yet you’re going through a divorce or you’re going through a tough time in life, or you have this pervasive mood disorder, and that’s the thing that’s up in the front seat, then we really want to get you the right care first. Because our brain gut behavioral therapies are not as effective if mood symptoms are not treated.
And that encompasses depression, but also, trauma. So, there’s a higher prevalence of trauma symptoms in patients that have GI conditions, and that alone can impact your digestive health and wellbeing.
And so, recognizing that if trauma remains untreated, then you’re going to have a harder time getting your GI symptoms under control. And so, it’s really been a part of my role to help educate people that things that are still with you, related to your mental health, we have to get that better controlled and we have to guide you to the right mental health expert for that.
So, that, I think is really important because sometimes patients will say, “Oh, I’ve been to a therapist before,” and not to discredit any of my mental health colleagues, but their treatment plans may look very different from somebody that is a GI psychologist and is going to jump in and address the IBS or whatever your GI condition may be.
So, if you’re contemplating working with a GI psychologist and you’ve never had access to that before, it is typically a bit different from more of a general mental health provider. So, we each play very important roles in people’s lives.
And I’ll also say that I have lots of patients that continue to work with their general mental health provider while they work with me. And I’m almost like the person that jumps in short-term. So, our behavioral therapies are usually anywhere from 1 to 3 to 5 to 10 sessions, and then we wrap up.
And so, it’s really about teaching the strategies and getting people access to the evidence-based care that helps them improve the way they’re coping and managing their digestive condition, and it’s not long-term therapy.
Melissa Joy (24:22):
That makes a lot of sense. Thank you. And I know I threw kind of two questions at you at once, but did you want to speak more about how stress impacts our physical health?
Megan Riehl (24:30):
Yeah. So, stress can produce different chemicals in our body. And a lot of us these days are just primed to have our body respond to different stressors in the same way that our body may respond to a lion, a tiger or a bear that could chase us.
So, our sympathetic system, which is your brain’s built in safety patrol to kind of keep you safe, which can activate your heart rate, it makes your breathing short and shallow. It can really lead to increased GI distress.
If that’s easily triggered by a thought of being at a concert and where am I going to go to the bathroom or driving in the car and getting a pang of urgency — when that system kind of revs up from whatever stressors are around us, it alters our gut motility. It produces different chemicals in our system and really, is a big target for the types of brain gut behavioral therapies that we teach people.
Melissa Joy (25:29):
Okay. Yeah, that makes a lot of sense. Should we transition more specifically into IBS now, and I have to say, you mentioned inflammatory bowel disease or IBD, and maybe it would be helpful to explain the difference between those two.
Megan Riehl (25:45):
So, inflammatory bowel disease is an organic disease where there are very objective biomarkers. They require typically medical management with a gastroenterologist. And until we find a cure, right now, it’s lifelong management with medication, patients can be prone to surgical intervention.
And what is similar about IBS and IBD is that both patient populations can benefit from a multidisciplinary team. Somebody that’s living with IBS may get almost complete alleviation of symptoms and or feeling extremely confident with the management of their condition with behavioral therapy or with a nutrition therapy.
In inflammatory bowel disease, a GI psychologist isn’t going to replace a medication. We don’t have a diet therapy at this point that’s going to replace a medication that helps keep a patient with IBD in remission.
So, very similar at times, symptoms, where a patient may experience abdominal pain, bowel fluctuation, but lots of other potential symptoms that can include joint pain, skin lesions, ulcerations from basically mouth to anus depending on the diagnosis.
So, I think that our book could certainly serve as a support for patients that have IBD, but we definitely highlight these are two very different diagnoses. And it’s very important for patients that think that they have IBS, if they’ve never had a consultation with a medical provider, we want you to see a doctor to get that definitive diagnosis.
Melissa Joy (27:29):
Okay. Very important. Yeah, I can imagine ruling out different things is complicated but important and could take time and a lot of probably delayed diagnoses or misdiagnoses along the way and all that stress involved.
So, let’s talk more about what IBS is and how does somebody develop it? What causes it?
Kate Scarlata (27:51):
Alright. Well, I’ll segue into this. So, it’s a chronic GI condition that presents with abdominal pain and alteration in bowel habits. So, some individuals are more prone to being constipated and they’d be IBS-C, we would call them. Or others have IBS-D, they’re more diarrhea predominant. There’s IBS-M, which is a mixed presentation. And also, U, which is unsubtyped, if we really can’t put someone in a box.
And then there’s also post-infectious IBS, which can occur after a bout of gastroenteritis. So, say an individual experienced foodborne illness with salmonella poisoning or norovirus is another example, and even some parasitic infections.
About 10 to 13% of those individuals that are affected with those conditions have severe gastroenteritis, will go on to have post-infectious IBS.
We don’t have a cure. We do not have a biomarker for IBS, it’s a symptom-based diagnosis. In that, we use to determine … after we’ve ruled out other things like IBD, et cetera, a patient will be diagnosed with IBS.
Melissa Joy (29:03):
Thank you. And I kind of mentioned misdiagnoses or delayed diagnosis. How do patients — how are they interacting with their healthcare providers on this? Are they seeking medical advice? Are they self-diagnosing? Are they open and interested in talking to their doctors about this?
Megan Riehl (29:21):
Yes, yes, and yes, and no, and yes. So, especially with IBS, there was a recent survey study that basically found that one in five patients with IBS didn’t want to talk to a medical provider or weren’t talking with a medical provider about this diagnosis. One in four were treating themselves with over-the-counter medications.
So, I think that even though we’ve come a long way from, “IBS is in your head, just stress less and you’ll be better. We’ve done a colonoscopy, endoscopy, there’s nothing there. Good luck, you’re fine” — we’ve come a little ways from that, but patients still feel this, and they still feel like they get the portal message that says your colonoscopy was unremarkable.
And I think because our medical system is so flooded where it could take six months or even a year to follow up with a gastroenterologist, a lot of these patients just feel a bit lost with where to go.
And so, that’s why they do, they turn to the over-the-counter medication or to the internet where Dr. Google is not our friend in some cases. There’s a lot, we call it snake oil in the book. And we kind of call out certain things that can be very dangerous for patients.
So, I’ll use an example of colonics. There are medi spas out there that will offer a coffee enema and a colonic, and your gut will be healed. And there are so many red flags in that we want people to be aware of.
Because when you don’t feel good, when it’s hard to get out of the door because you’re pooping so many times, or you have the urge to go and you can’t go and you have abdominal pain and bloating, you are willing to spend your last dime sometimes or rack up credit card bills in order to feel better for these offhanded cures.
So, we say, if anybody’s offering you a cure for IBS, it’s BS in a lot of ways.
Melissa Joy (31:35):
Run the other way.
Megan Riehl (31:37):
Yeah. And so, we just want to be mindful of that and fill people with the science-based strategies to help them feel better.
Melissa Joy (31:44):
Yeah, I can imagine a lot of people are desperate. And I know that’s one of the reasons I became a … well, one of the reasons I enjoy being a diabetes educator is because there are a lot of opportunities for people to just desperately seek some kind of solution. And I feel they’re taken advantage of by a lot of products and gimmicks, I guess, would be the word.
Megan Riehl (32:08):
A lot of these patients will say, “I wish they would find cancer or …” and they’ll say, “As terrible as this sounds, at least that would be something we could try and cure, and I’ll take chemo.” And I know that that’s a really kind of shocking thing to say, but this patient population is really suffering.
So, when we say there’s “nothing wrong with you,” it really invalidates their experience. Because on a day-to-day basis, there is something, it’s hard to get to work, it’s hard to socialize, it’s hard to eat.
And so, I know that my dietitian colleagues and myself and a gastroenterologist will say, “We know what this is. This isn’t easy, but we know what this is, and we can work together with you to create a plan.
And with that plan, our goal is that when, and if you have symptoms, the duration of those symptoms, the severity of those symptoms, the frequency of those symptoms, we can make all of that better with these strategies. It’s just going to take us some time.”
Melissa Joy (33:13):
Yeah. Well, maybe that’s a good segue into talking about some of what’s in the book, because I know that it starts off talking about the gut brain connection or actually the gut brain and food connection. I know that there’s nutritional remedies in there, there’s symptom specific intervention.
And obviously, we can’t cover everything in the next 15, 20 minutes, but would love to hear maybe some of what’s in the book and some things that would be helpful for most people listening to at least kind of give them a framework or a foundation to start with. And then maybe we can dig into a couple of the other specifics.
Kate Scarlata (33:50):
Sure. So, we start off the book really talking about what the gut brain connection is, how food might trigger symptoms in someone with IBS, and really break down the variety of different ways that these interactions can impact their symptoms.
And really, try to help the patient identify, “That’s me.” Because you might not have stress-induced IBS, you may be more of a microbiome diet IBS-er, and the diet pieces will make a lot more sense to you. And sometimes, it’s both. And sometimes it’s, “I am a definitely stress-induced IBS-er.”
So, we’re kind really setting the stage for how stress can impact your symptoms. We know that it increases GI motility, it can affect even these immune cells getting activated in the gut, releasing inflammatory chemicals that are right next to the nerves, really increasing the sensation, the visceral hypersensitivity, we call it. It’s sensitivity to pain in the gut.
That’s all starts with stress, but yet, it has these physical effects. And we know that certain food items can trigger mucus secretion, intestinal permeability. We see FODMAPs for instance, pulling in water to the gut, which stretches the gut and are fast food for our gut microbes that love them and create copious amounts of gas, which a lot of patients experience and can trigger cramping, et cetera.
So, in the beginning, we’re kind of setting those stages and really outlining a number of different interactions. And then we really dive into … and I’ll let Megan kind of intercept because the first few chapters are all about mind-gut connection. So, I don’t know if you want to talk about that, Megan, and then I can come back.
Megan Riehl (35:41):
Sure. So, we wanted to provide tangible resources for our readers. And so, I cover first, some outlines of how our brain and gut are communicating and connecting.
And then we dive into relaxation-based strategies. So, helping people to understand that by relaxing their body, this is very helpful for relaxing their gut and giving very gut directed relaxation strategies. So, there’s a relaxation chapter.
There’s a chapter that outlines the use of really what comes from cognitive behavioral therapy, which is CBT. And in our world of brain gut behavioral therapies, we take that CBT and hone it into gastroenterology.
And that means that a lot of our patients avoid things because of their anxiety related to their digestive condition. And that avoidance, we think it’s protective, but it actually just makes things worse. So, we outlined some ways to utilize some CBT strategies such as a thought record, which outlined the pathway of thinking differently. And we call that cognitive restructuring.
So, we take some of these CBT techniques and make them introductory in a way, which also then kind of guides us to helping people to understand, hey, this is just 101. And if you’re interested in learning more or diving deeper, you might consider working with a GI psychologist or maybe you’ve identified a general mental health provider is really what I need right now.
So, these chapters are tangible resources, you will definitely walk away with something that you can practice in the first couple pages, and also, it’s written in a way that you want to go back. So, we’ve even created kind of a strategies tracker in the book so that as you’re reading along, you can write down, “I really liked the diaphragmatic breathing section, and that’s on page X, and I’m going to go back to that one.” So, we set you up for success so that you can go back to things.
Kate Scarlata (37:53):
I found Megan’s chapters really helpful and was sharing them with family members just because they’re so appropriate for really any of us. Very helpful, relaxation, mindful minute, lots of just tips that any one of us could really embrace in our daily life.
So, moving on, after we do a lot of behavioral therapies and introduction to the gut-brain connection, we move into evidence-based nutrition therapies. And I’m a big believer that the least restrictive diet possible to help you manage symptoms is always the goal.
We’re not going for these strict, ridiculous diets right from the get-go if we don’t need to. And certainly, some people need the real strict diets, and a dietitian can help guide if that’s the right choice.
So, we start with a gentle diet cleanup where we’re really looking at some of the major, well-known IBS triggers: too much alcohol. We know too much alcohol and too much caffeine, even if you don’t have IBS, can trigger symptoms.
So, we’re really just looking at some of these overindulgences and how to kind of clean up the diet a little bit. It’s based on an outline of the UK traditional dietary advice called the NICE guidelines, which has evidence to support its use in IBS as being beneficial. Not for all, not as good as the low-FODMAP diet, but a good first start.
And then I go into what we call the low-FODMAP elimination diet, which is the traditional low-FODMAP diet. Just for your listeners, FODMAPs, it’s an acronym that stands for fermentable oligosaccharides, disaccharides, monosaccharides, and polyols.
Don’t worry, you don’t need to memorize these, but they’re short chain carbohydrates that are commonly malabsorbed and can trigger IBS symptoms. And we’ll do the elimination phase outline in the book.
And then we do a more gentle approach, the FODMAP gentle approach, which is just a drilled down version, just a looser version, what we call a bottom-up approach where we’re just cherry-picking out some high-FODMAP foods, not putting someone on a strict elimination diet.
I do that a lot in clinical practice right now, very helpful. We need a little more data on that. It’s being studied right now, but it’s also very effective from my clinical experience.
So, we kind of outline those diet interventions in chapter five, along with the next chapter really covering all the details, label reading, menu planning, all the things you need to actually apply these diets. So, you have all the tools in the absence of having a dietitian, but you can also certainly use the book alongside your dietitian as well.
Melissa Joy (40:39):
Yeah. And I know when we talked about FODMAPs before, and even just digestive health in general, and I appreciate your approach about let’s have the least restrictive diet possible, because some of the foods that can be triggering are healthy, nutritious foods. It’s not like we can just say it’s all alcohol or what was the other-
Kate Scarlata (41:00):
Caffeine.
Melissa Joy (41:01):
Caffeine. It’s things that we can really live without, maybe. We don’t want to restrict foods unless they are causing problems. So, that’s where that sort of elimination phase and then reintroduction phase and so on.
And then I know that there’s also a chapter on (which I love the way this is phrased, and you could just touch on briefly maybe) Making Sane Food Choices in a Food Fear and Weight Obsessed Culture. Why did you decide to include that aspect? I mean, I know that we’re all impacted by that, but I guess it’s just another layer for people with IBS.
Kate Scarlata (41:39):
Absolutely. So, that was very important to me, and we had to be very sensitive with this topic because we really talked a lot about sort of the emerging research that we’re seeing in GI conditions with the higher risk of disordered eating, almost a quarter of patients with GI conditions display disordered eating.
We’re really trying to delve into this connection a little bit better because certainly, if you’re eating and it’s painful and 90% of IBS patients say that food triggers their symptoms. So, there is an adaptive response to pulling back on food. It’s just that when that adaptive response and those food lists come down to six or five foods, then it’s really impacting nutrition, quality of life, mental health and other areas.
So, we wanted to talk about this aspect because of the link with the disordered eating and IBS. But also, we know that people that have eating disorders, about 52% of them fit the criteria for having IBS as well. So, this restricted eating also can cause IBS symptoms, and then IBS can also lead to restricted eating.
So, it needs to be said, but then we also live in this emerging world where food fear is so abundant on our TikTok, social media channels. And I know there’s a lot of dietitians doing a lot of great work to debunk these crazy messages, but this is what people are hearing that don’t have sound nutrition degrees. And like Dr. Riehl mentioned earlier, when you’re feeling miserable, you’ll fall for that snake oil, it’s very easy to.
So, we wanted to really bring up this subject as thoughtfully as possible. Disordered eating may be emerging here if you’re concerned about that. And just this link with social media use and otherwise that are also contributing to this issue.
Melissa Joy (43:47):
Yeah, that makes me wonder about all the pseudoscience that’s out there in social media as you mentioned. Are there some common myths that you’re seeing percolate to the surface that you’d like to address?
Megan Riehl (43:59):
Well, I mentioned one earlier that IBS is curable. And the reality is that we want to reduce your symptoms and the frequency of how often you’re flaring, but mostly, we want to empower you with strategies in your toolbox.
And so, if you are having a lot of symptoms, then you might need to go to a bit of a gentle diet for a couple days, but we don’t want you to restrict your food for the rest of the month, and that you may incorporate some of our behavioral strategies while your stomach kind of settles back down.
So, I think that the reality is we can help you, it oftentimes is just, it might be that you need another team member, and that it is a pretty wide spectrum of specialties that can help with your IBS.
So, for example, pelvic floor physical therapists, a lot of our patients would never even consider a physical therapist a part of their team. But this can have a tremendous impact on patients.
And yet, again, similarly to some access issues with a GI dietitian or a GI psychologist, a lot of times there’s just this lack of information about the different team members that are out there. And so, when we’re thinking about the dream team, like we call it, in order to manage your IBS, it just might include a lot more members than you would’ve thought.
Melissa Joy (45:26):
Or maybe not even realize exist.
Megan Riehl (45:28):
Exactly.
Melissa Joy (45:29):
Any other myths you want to address? I know you had mentioned cleanses before.
Megan Riehl (45:34):
Yeah. Again, if you need a colonic, you need to talk to your gastroenterologist because doing a colonoscopy is essentially a colonic. So, if you’ve done a recent colonoscopy and you’ve received a definitive diagnosis from your gastroenterologist, we don’t need you paying for juice cleanses.
And to Kate’s point, sometimes, the juice cleanse that you’re finding on the internet is filled with high-FODMAP of fruits and vegetables. And so, it ends up doing far more damage than it’s going to do you good. And then you’re just going to be hungry, hungry and your symptoms persist.
So, you really need to talk to a registered dietitian, a licensed registered dietitian, a licensed GI psychologist, a gastroenterologist that is willing to talk about the science behind the reason that they’re making a recommendation.
And there are some incredible naturopathic doctors out there who might make a recommendation for a supplement or a probiotic. And I think that if that is a part of your team, you want to talk with them about the science behind why they’re making that recommendation.
So, before you go and shell out $1,500 for a supplement regimen, ask about what’s the science that backs this recommendation before you go ahead and pursue that.
Kate Scarlata (47:00):
And I would just say one more. There is no set IBS protocol. We hear this a lot: “My IBS protocol cures IBS.” And IBS is so heterogeneous because some people will have stress-induced IBS, some people will be diet induced, some people have constipation, some people have mixed presentations, some people have diarrhea.
There is no one size fits all approach to IBS. And so, when they have their protocol to get at the root cause of your IBS, walk away.
Melissa Joy (47:36):
Good advice. Well, that leads me to think about are there some things whether it’s diet, nutrition, lifestyle that anyone could do to improve gut health and also maybe an opportunity for you to speak to what you’re seeing in the science now with regard to maybe specific foods or food groups. Any interesting research that you wanted to share on that.
Kate Scarlata (47:57):
Yeah, I can speak to that. I will say the gut health area and the trillions of microbes that live in our gut, it’s very complicated. So, I think people want to drill this down into simple bites or the media takes something and rolls with it. And it’s not quite that exciting, if you’re really looking at the science critically.
But I will speak to a couple studies. So, the American Gut Project is a crowdfunded stool bank. And they analyze stool and look at different types of microbes and different types of metabolites. Kind of get a sense, they also have individuals send in food diaries so they can look at what they’re eating and relate that to what they’re finding in their stool microbiome.
And in one of their studies, they did find that in individuals that were eating 30 different types of plant foods versus those that were having 10 or less, that those that had the variety of plants in their diet, they had greater microbial diversity. And that is a marker of better gut health. We believe the variety of microbes there is a good signal. So, there’s that study.
Another study that got a lot of press was from Stanford University. And this was a teeny weenie study. I think they had maybe 13 in each arm. And what they did was they looked at individuals on a very high fiber diet, 40 grams per day, and another group looking at fermented foods.
And all the fermented foods that they provided had live and active cultures. And there were six servings of fermented foods every day. So, this is pretty significant, not typical of what people do eat.
But what they found was in the fermented food arm, they had greater microbial diversity and had some inflammatory markers, protein markers that were reduced. One of the markers was interleukin 6, which is associated with diabetes and rheumatoid arthritis.
So, again, signals that fermented foods, especially those with live and active cultures, may have beneficial effects on microbial diversity.
Megan Riehl (50:13):
So, I think from a behavioral perspective, what can people do? And just a general healthy lifestyle is the goal. And I say that knowing that it can be a privilege to have a healthy lifestyle, period — in America, throughout our world.
But if you have access to clean air, getting outside, going for a walk, getting some sunshine, these are things that I think people are like, “Really? Is that going to make a difference? I mean, that sounds a little woo-woo.”
But it does, it helps to neutralize stress hormones in our body. Again, it doesn’t mean that you have to have an expensive gym membership and get to the gym every single day. A 20-minute walk to get your heart rate up can be something that’s tangible and that you can set a goal for.
And that’s really, I think one of the takeaways from the book here too, is, as Kate said earlier, a lot of the behavioral strategies that I mentioned in those chapters are things that are good for just general mental health, general wellness.
We all can benefit from learning how to do diaphragmatic breathing, so that after we’ve had a tense conversation with a colleague or a difficult situation at work or school, kind of taking some time for self-care and regulating your body, your breathing, reducing muscle tension — that’s going to help you come back to whatever is in front of you with a bit of a more clear head and maybe a gut that’s not as agitated.
So, I think that finding the strategies that are of interest to you, we make that point too in the book that if running is not your jam, then have a sit down with yourself and say, “What am I really interested in? Do I like to dance? Do I like to walk? Am I more likely to do something if I have somebody to hold me accountable? Can I get out and walk with a neighbor or a family member?”
Is this something from a lifestyle perspective and from a value, what do you value? And we give some guidance on determining what do you value in the book. And if health is one that hasn’t been a high priority for you until maybe you got an IBS diagnosis, we highlight that that can shift, that can shift as time goes on and with interest the increase.
So, I think finding that balance of what you’re interested in, what you’re motivated in, and also trickling it down to the family that what we model for our kids makes a big difference. And we can shape those little guts by what we do as adults within our home.
Melissa Joy (52:51):
Very good. I love that you mentioned the value because I think really getting down to the value is key for long-term behavior change and it’s very powerful. So, that’s exciting that that’s in there as well.
Is there anything else that you want to share with us about gut health, IBS, something in the book, or maybe some takeaways for the audience just as we’re wrapping up?
Kate Scarlata (53:15):
Eat more plants, relax, get good sleep. You did not cause IBS. I think there’s a lot of guilt with this diagnosis, which is completely unnecessary. And you don’t need to be perfect. I think everyone’s trying to follow the rules.
And really, even with the low-FODMAP adjustments, I’m always saying to my patients, “This isn’t about eliminating FODMAPs or being perfect on the diet because that’s too stressful. It’s just about modifying, moving, stepping in the right direction.”
I think we put a lot of pressure on ourselves and our kids sometimes as a general rule, and we just need to relax a little bit more and it’s not a sprint, it’s a marathon. Patience is really important. Get you a dream team and you can make a difference in the way you feel.
Melissa Joy (54:06):
Great. And Megan?
Megan Riehl (54:08):
The only thing I’ll add is just that you deserve to live well, and that you can. And so, if you’re not there yet, then Mind Your Gut is a good place to start.
And I’ll segue to another shameless plug. We have a podcast that focuses on gut health. So, literally, it’s The Gut Health Podcast. And we just launched it again, because we’re like, “Alright, we’ve written the book, and now, how do we keep this conversation going?” Because gut health is important for not just those people that have IBS, it’s for people that haven’t been diagnosed with a GI condition and/or don’t have a GI condition.
But it goes back to kind of where we started today’s episode with gut health matters for everyone. And so, we wanted to explore more aspects of that, and we do that in the podcast.
Melissa Joy (54:56):
Excellent. Congratulations on the launch of that new podcast. And I haven’t tuned in yet, but I plan to.
You also have a couple other interesting things that you’re working on that I’d love for you to share, and also, where people can find more information, following you on social. Share whatever you want now. And of course, I’ll have all the links in my show notes at soundbitesrd.com.
Kate Scarlata (55:18):
Sure. So, you can continue this conversation regarding the book at our Instagram handle at mindyourgutofficial. Megan and I both have Instagram handles that we’re fairly active on at Kate Scarlata and at Dr. Riehl.
Megan and I have worked together for those dietitians that may be listening on a CEU program with Today’s Dietitian. And it utilizes our book, Mind Your Gut. And so, that’ll be forthcoming. I think that’s going to be released sometime April, May of 2024, so be on the lookout for that as well.
Megan Riehl (55:50):
And you can pick up our book really wherever books are sold. So, Amazon can next day it to you, tomorrow. And we also would love you to support your local bookstore.
So, the other thing I will just also say is that the book comes in hard copy, but we also have an audiobook. And the cool part about the audiobook is the relaxation strategies that are explained in the book are beautifully narrated in our audiobook. So, you get to kind of listen if you have the audiobook. So, it’s kind of another offering.
Melissa Joy (56:22):
Excellent. Thank you for sharing all of that information. And like I said, I’ll have the links in my show notes as well at soundbitesrd.com.
Thank you both so much for all this important work that you’re doing and for sharing it with us today on the podcast.
Kate Scarlata (56:35):
Thanks for having us.
Megan Riehl (56:37):
Thank you for having us.
Melissa Joy (56:38):
And for everybody listening, if you like this episode, please share it with a friend, tell a friend about the podcast. And as always, enjoy your food with health in mind, and with gut health in mind. Until next time.
[Music Playing]
Voiceover (57:53):
For more information, visit soundbitesrd.com. This podcast does not provide medical advice. It is for informational purposes only. Please see a registered dietitian for individualized advice.
Music by Dave Birk, produced by JAG in Detroit Podcasts. Copyright, Sound Bites, Inc. All rights reserved.
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
Hi Cindy,
Episode 262 has not been submitted for CEUs. Only select episodes are submitted for CEUs. You can check my Free CEU page here to see what episodes are available, when they expire and to access the CEU activity/quiz: https://soundbitesrd.com/sound-bites-podcast-free-ceus/. There you will find a long list of Free CEU activities including Ethics CEUs.
Hope this helps! Thanks for listening to my podcast.
Melissa
Hi Cindy,
This episode has not been submitted for CEUs but there will be a CEU opportunity for this topic through Today’s Dietitian soon.
Please visit the Today’s Dietitian site here: https://www.todaysdietitian.com/cell.shtml or check back to this shownotes page for updates when they are available.
Also – please note that not every episode gets submitted for CEUs and you can always check my CEU page to see what is available and when they expire: https://soundbitesrd.com/sound-bites-podcast-free-ceus/
Thank you,
Melissa
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
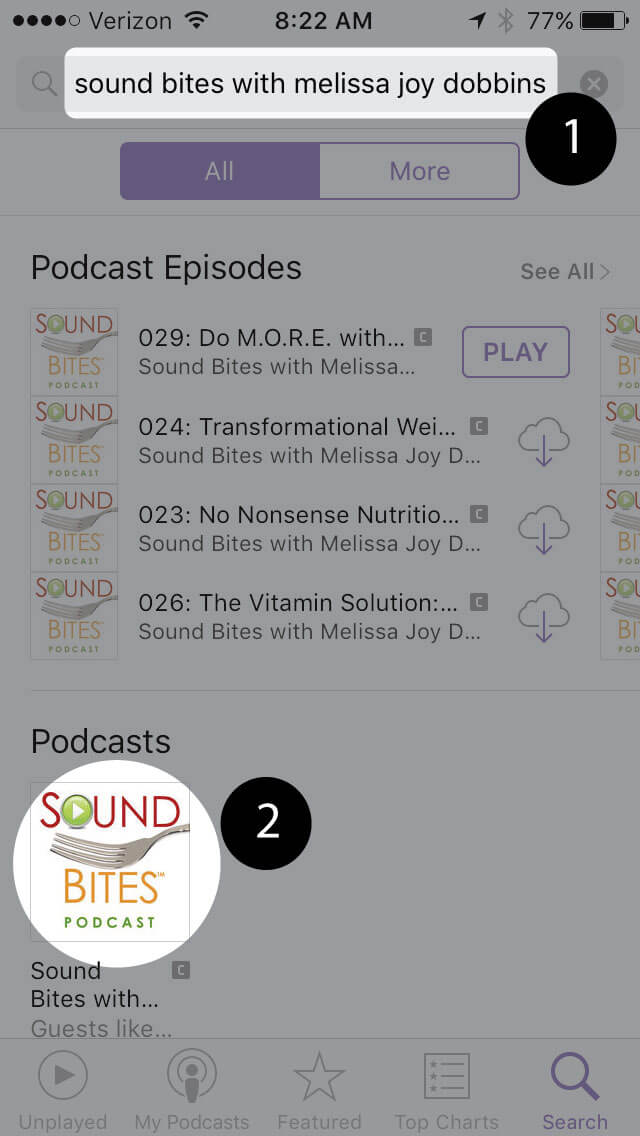
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
How to subscribe via iTunes
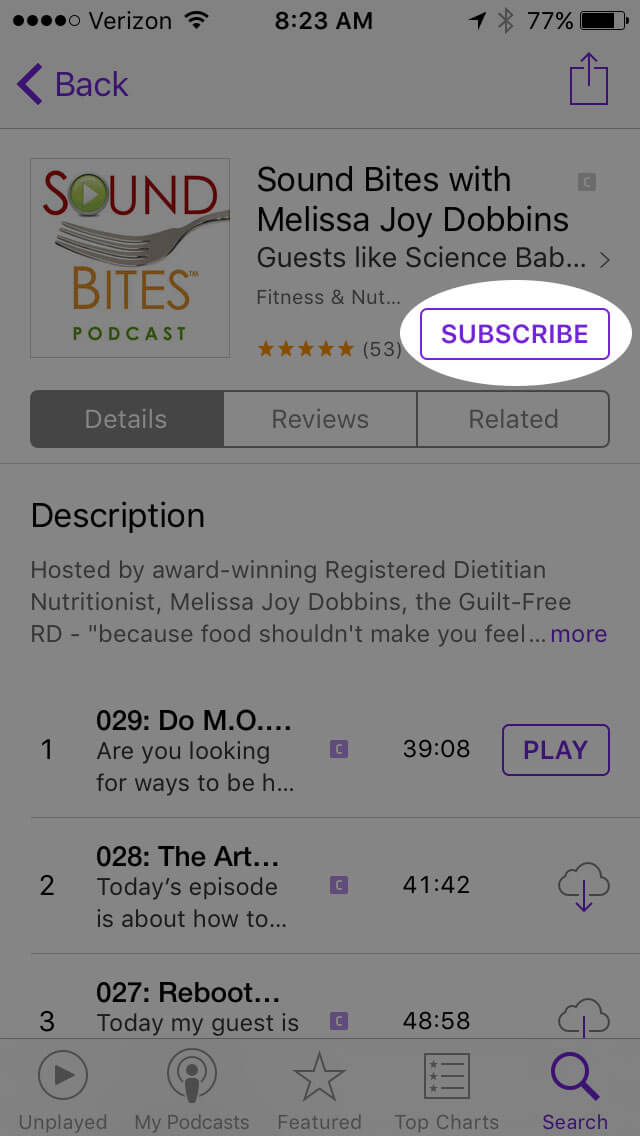
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!
Click “View in iTunes”
Click “Subscribe”
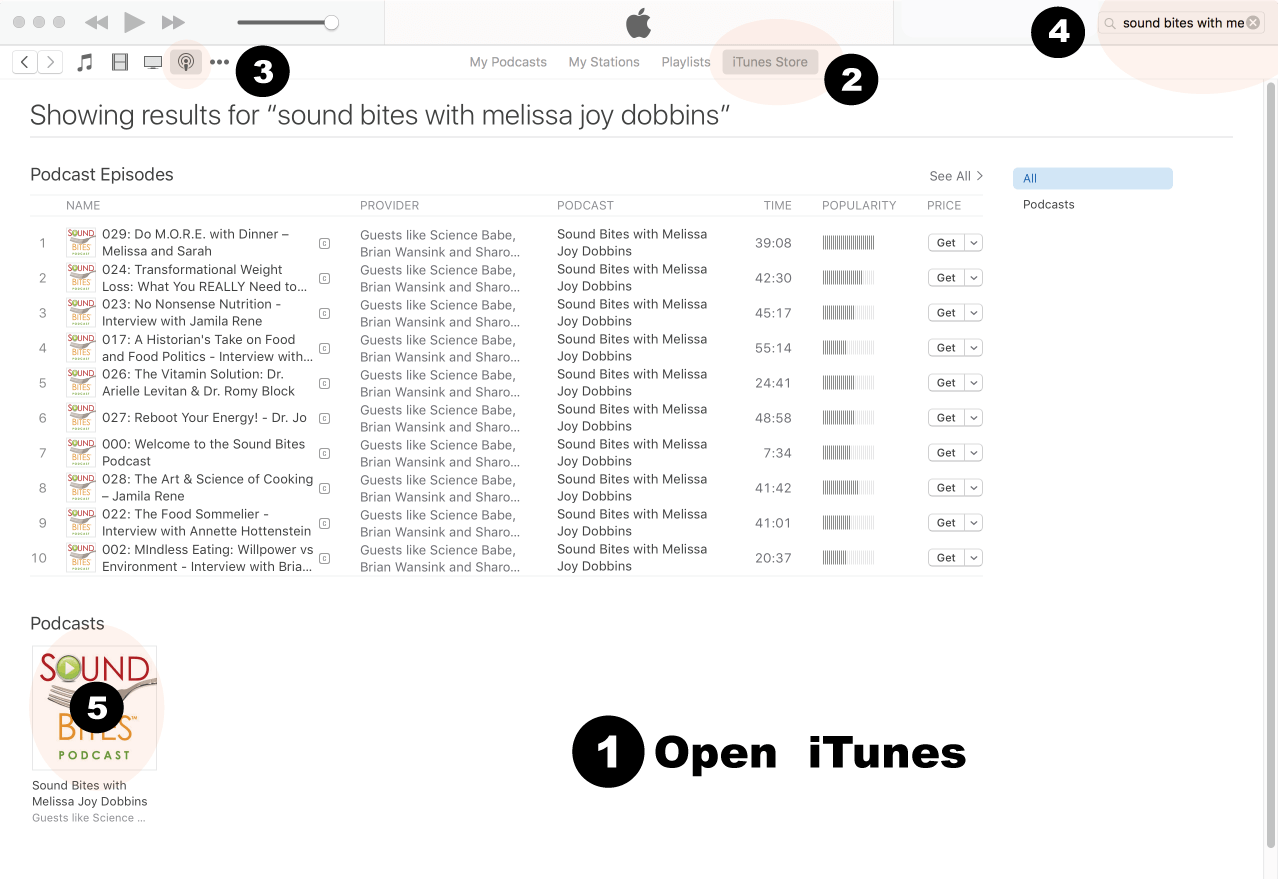
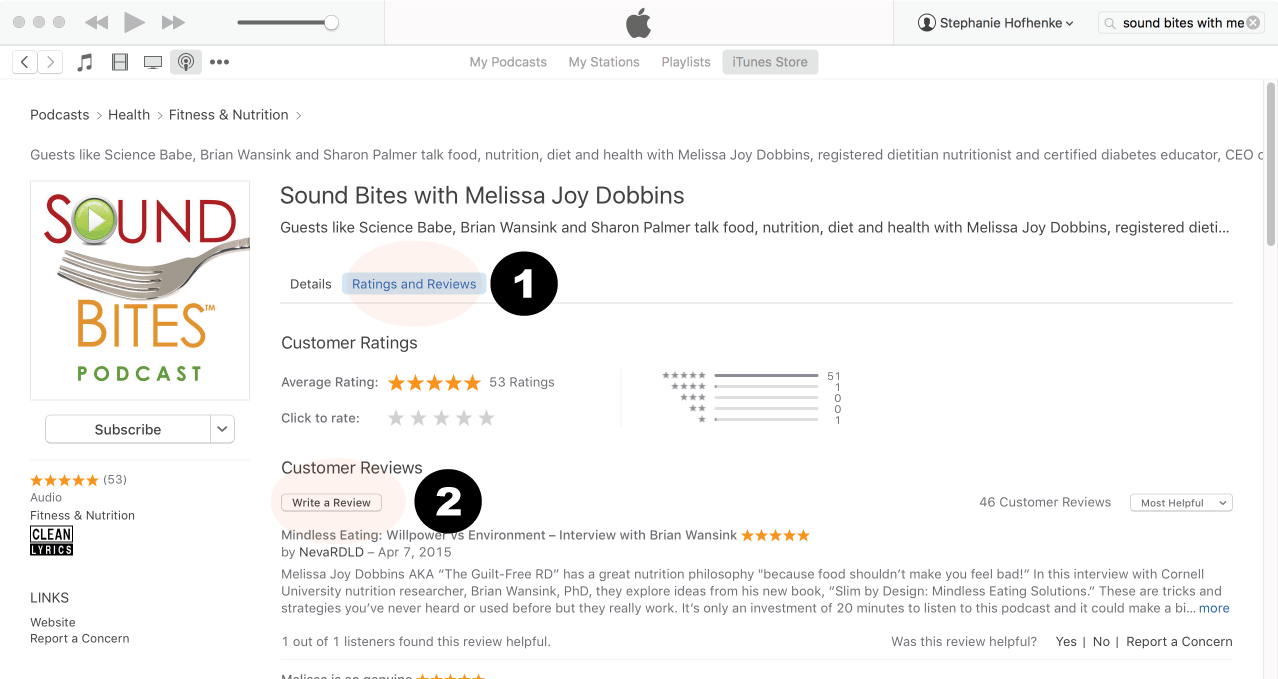
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
Click on podcast image
Search for Sound Bites podcast in iTunes
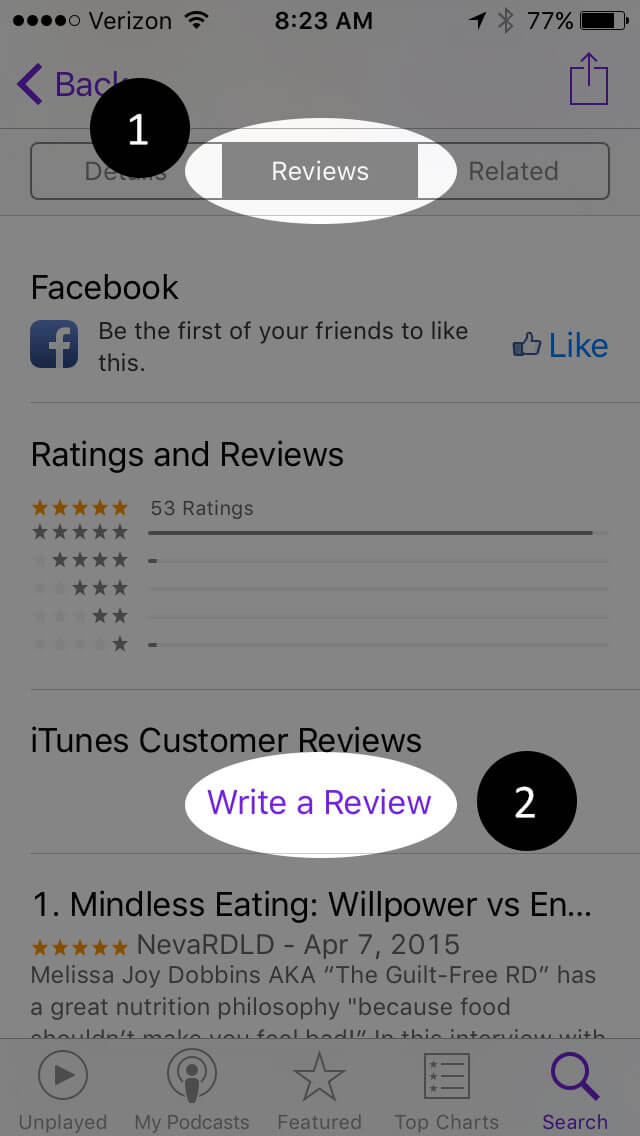
Click Ratings & Reivews
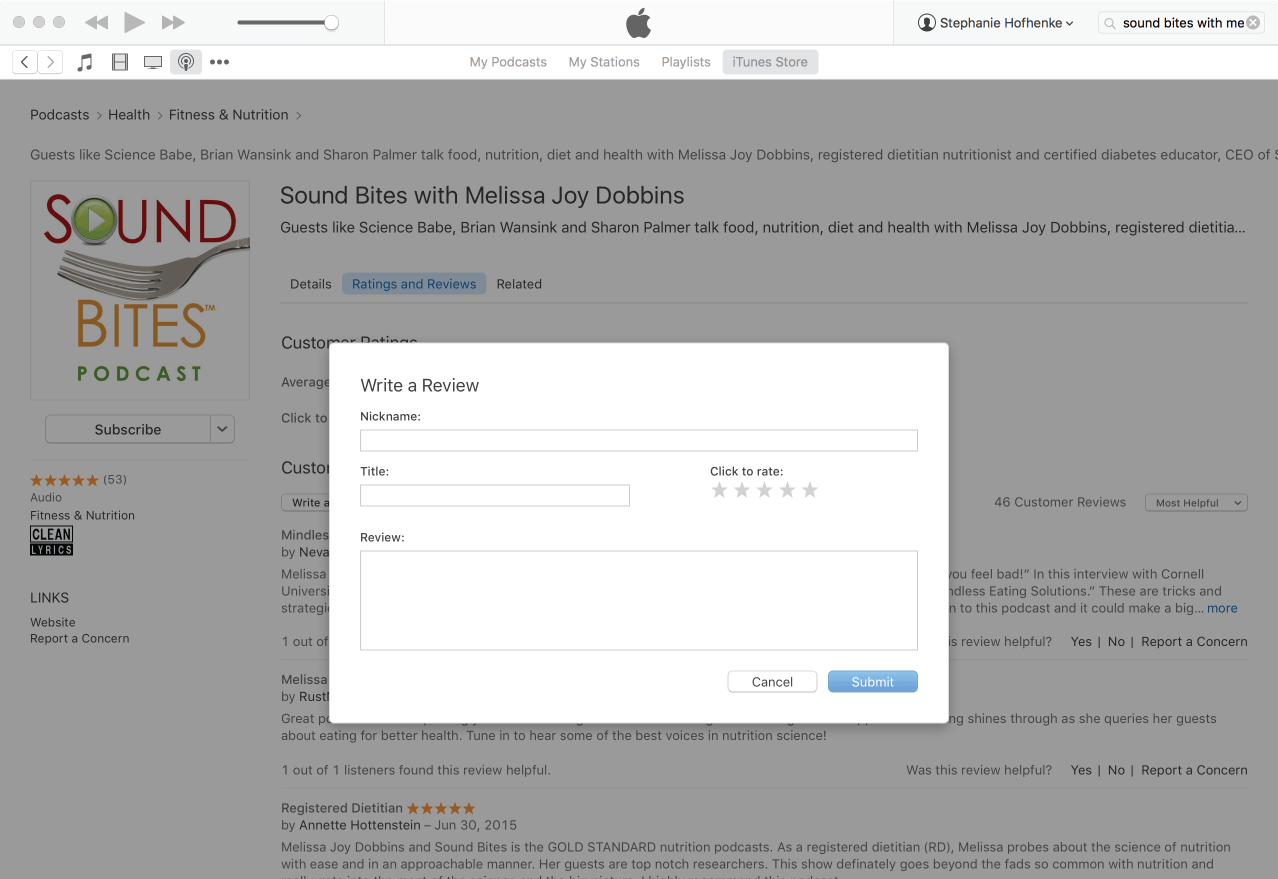
Click Write a Review
View reviews and write your own review.
Write your review…. Thank you!
Write your review!
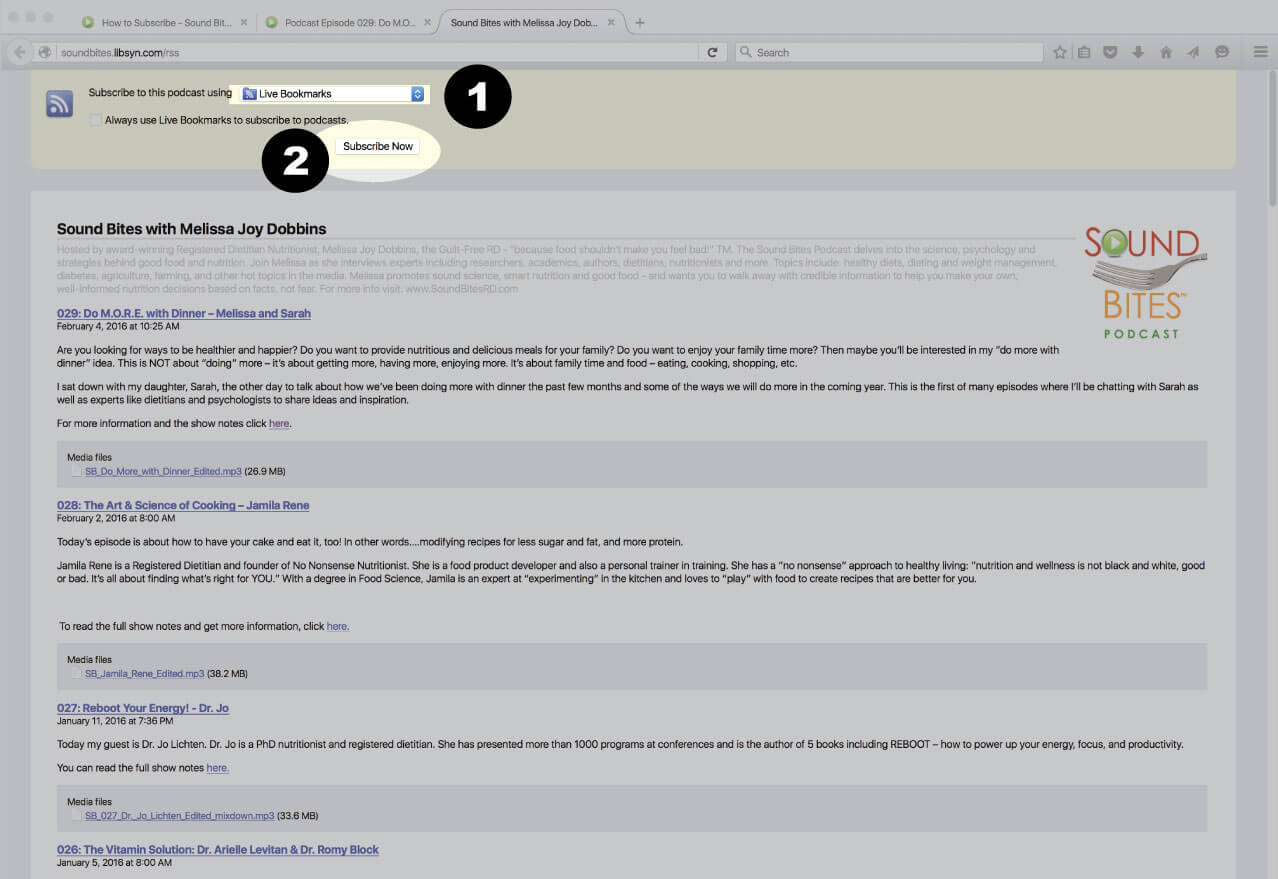
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
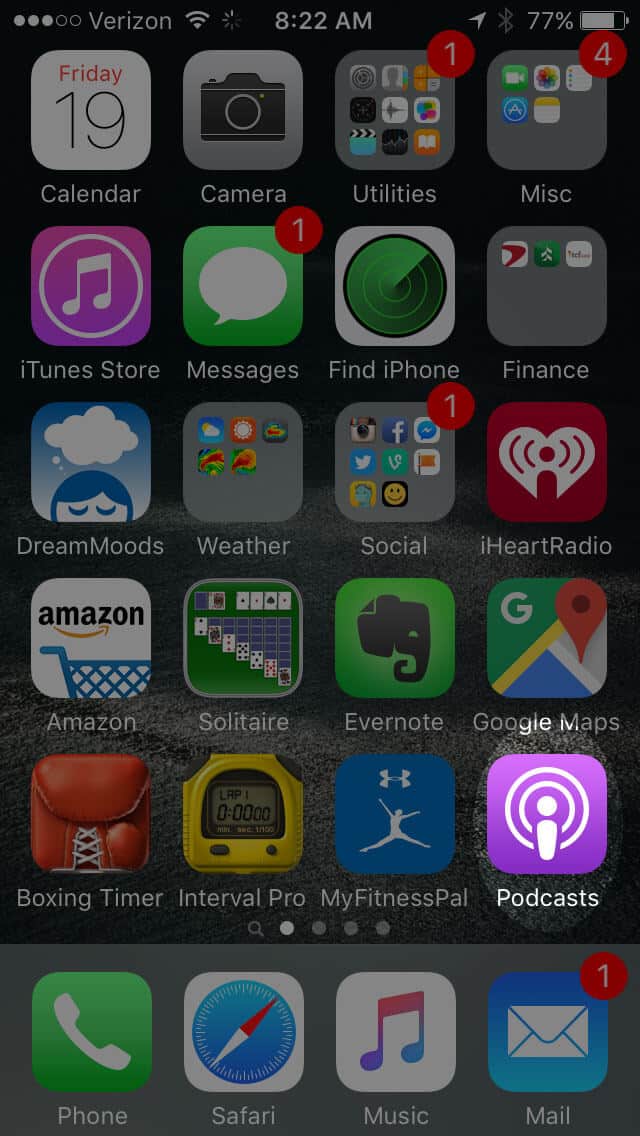
Subscribe & Review on iPhone
Open the “Podcast” app on your iPhone
Search for “Sound bites with melissa joy dobbins”
Open the podcast and click “Subscribe” and your done!

 This episode is not available for CEUs through the Sound Bites Podcast. However, there will be a CEU opportunity available through Today’s Dietitian in the near future. Please visit the Today’s Dietitian site or check back here for further details to be shared when they are available.
This episode is not available for CEUs through the Sound Bites Podcast. However, there will be a CEU opportunity available through Today’s Dietitian in the near future. Please visit the Today’s Dietitian site or check back here for further details to be shared when they are available. Dr. Megan Riehl is an Associate Professor of Medicine and Director of GI Behavioral Health at the University of Michigan where she has a full-time clinical practice, leads GI behavioral health trainings, and provides mentorship and consultation. Her clinical expertise spans the field of gastroenterology from those living with IBS to those with chronic gastrointestinal diseases. Dr. Riehl actively engages on multiple national committees focused on improving the psychological well-being of individuals with GI conditions. Her research and passion for education has resulted in numerous peer-reviewed publications, leadership roles, and international speaking engagements.
Dr. Megan Riehl is an Associate Professor of Medicine and Director of GI Behavioral Health at the University of Michigan where she has a full-time clinical practice, leads GI behavioral health trainings, and provides mentorship and consultation. Her clinical expertise spans the field of gastroenterology from those living with IBS to those with chronic gastrointestinal diseases. Dr. Riehl actively engages on multiple national committees focused on improving the psychological well-being of individuals with GI conditions. Her research and passion for education has resulted in numerous peer-reviewed publications, leadership roles, and international speaking engagements. Kate Scarlata is a US-based dietitian with 30+ years of clinical experience. Kate’s expertise is in gastrointestinal disorders and food intolerance. She was awarded the Outstanding Massachusetts Dietitian Award and recognized as Boston’s Best Dietitian by Boston Magazine. Kate is the co-author of numerous books and articles on digestive health topics including Mind Your Gut with Dr. Megan Riehl (pub date March 5, 2024), the New York Times Best Seller, The 21 Day Tummy Diet, and The Low FODMAP Diet Step by Step. Kate completed her postgraduate training at Brigham and Women’s Hospital, a Harvard Medical School teaching affiliate, and her master’s degree in public health at University of Massachusetts. In addition to her clinical work, Kate’s patient advocacy work includes her #IBelieveinyourStory campaign raising awareness of IBS, sharing patient’s lived experiences, and securing funding for IBS research as well as her #EndHungerPain initiative where Kate partnered with food manufacturers to provide special diet foods to food pantries. The #EndHungerPain initiative increased attention to the many challenges of living at the intersection of gluten free and low FODMAP diet needs while food insecure.
Kate Scarlata is a US-based dietitian with 30+ years of clinical experience. Kate’s expertise is in gastrointestinal disorders and food intolerance. She was awarded the Outstanding Massachusetts Dietitian Award and recognized as Boston’s Best Dietitian by Boston Magazine. Kate is the co-author of numerous books and articles on digestive health topics including Mind Your Gut with Dr. Megan Riehl (pub date March 5, 2024), the New York Times Best Seller, The 21 Day Tummy Diet, and The Low FODMAP Diet Step by Step. Kate completed her postgraduate training at Brigham and Women’s Hospital, a Harvard Medical School teaching affiliate, and her master’s degree in public health at University of Massachusetts. In addition to her clinical work, Kate’s patient advocacy work includes her #IBelieveinyourStory campaign raising awareness of IBS, sharing patient’s lived experiences, and securing funding for IBS research as well as her #EndHungerPain initiative where Kate partnered with food manufacturers to provide special diet foods to food pantries. The #EndHungerPain initiative increased attention to the many challenges of living at the intersection of gluten free and low FODMAP diet needs while food insecure.











Does podcast 262 Mind Gut podcast qualify for RD CEUs?
I can’t find a quiz to take.
Cindy Benedict RDN LDN
Hi Cindy,
Episode 262 has not been submitted for CEUs. Only select episodes are submitted for CEUs. You can check my Free CEU page here to see what episodes are available, when they expire and to access the CEU activity/quiz: https://soundbitesrd.com/sound-bites-podcast-free-ceus/. There you will find a long list of Free CEU activities including Ethics CEUs.
Hope this helps! Thanks for listening to my podcast.
Melissa
Hi Cindy,
This episode has not been submitted for CEUs but there will be a CEU opportunity for this topic through Today’s Dietitian soon.
Please visit the Today’s Dietitian site here: https://www.todaysdietitian.com/cell.shtml or check back to this shownotes page for updates when they are available.
Also – please note that not every episode gets submitted for CEUs and you can always check my CEU page to see what is available and when they expire: https://soundbitesrd.com/sound-bites-podcast-free-ceus/
Thank you,
Melissa